

#NephMadness Choosing Wisely Campaign: Trial Outcomes Region #TrialsRegion
 Welcome to the #TrialsRegion; the region with the greatest potential for generating debate about clinical practice (in my humble opinion). Our ability to distil out the relevant information from the outcomes of trials is paramount in improving the delivery of care to patients with kidney disease. Particularly given the rising prevalence of CKD, there is a clear imperative to develop additional therapies through high-quality trials. Much focus has been placed upon the quality and quantity of RCTs within Nephrology; the overall consensus is that we are lagging behind other specialities. Selection of the correct surrogate marker is fundamental in determining the relevance and wider applicability of trial outcomes.The first matchup in this region pits the old familiar reliable against the young pretender.
Welcome to the #TrialsRegion; the region with the greatest potential for generating debate about clinical practice (in my humble opinion). Our ability to distil out the relevant information from the outcomes of trials is paramount in improving the delivery of care to patients with kidney disease. Particularly given the rising prevalence of CKD, there is a clear imperative to develop additional therapies through high-quality trials. Much focus has been placed upon the quality and quantity of RCTs within Nephrology; the overall consensus is that we are lagging behind other specialities. Selection of the correct surrogate marker is fundamental in determining the relevance and wider applicability of trial outcomes.The first matchup in this region pits the old familiar reliable against the young pretender. Doubling of creatinine has been used as an endpoint in randomised clinical trials for decades. Long-term changes in serum creatinine are thought to reflect a structural renal function decline and predicts development of ESRD. Doubling of creatinine should reflect a sustained reduction in GFR and represent an important step in progression to ESRD.Although well established, this venerable contender is far from flawless. Using the CKD-EPI creatinine equation a doubling of serum creatinine level approximately corresponds to a 57% decline in eGFR based on serum creatinine level which is a relatively late outcome in CKD. The variable acute and chronic effects of many drugs on renal function suggest caution should be used when interpreting clinical drug trials using doubling of serum creatinine as outcome.Enter the challenger 40% reduction in eGFR. There is great interest in considering alternative endpoints to shorten trial duration and reduce sample size. 40% is obvious less than 57%, meaning you hit your clinical endpoint at an earlier stage. This has significant implications for the design and likely successful outcomes of CKD trails. Unfortunately, CKD does not decline in a step-wise manner which is a significant limitation of this approach. Steady loss of function over time is a relatively late manifestation that reflects physiological factors in remnant nephrons. The applicability of 40% decline in eGFR is not uniform across all clinical settings, particularly if the treatment effect is not uniform across those who progress rapidly and those who do not progress. The use of different equations for determining eGFR must also be consider
Doubling of creatinine has been used as an endpoint in randomised clinical trials for decades. Long-term changes in serum creatinine are thought to reflect a structural renal function decline and predicts development of ESRD. Doubling of creatinine should reflect a sustained reduction in GFR and represent an important step in progression to ESRD.Although well established, this venerable contender is far from flawless. Using the CKD-EPI creatinine equation a doubling of serum creatinine level approximately corresponds to a 57% decline in eGFR based on serum creatinine level which is a relatively late outcome in CKD. The variable acute and chronic effects of many drugs on renal function suggest caution should be used when interpreting clinical drug trials using doubling of serum creatinine as outcome.Enter the challenger 40% reduction in eGFR. There is great interest in considering alternative endpoints to shorten trial duration and reduce sample size. 40% is obvious less than 57%, meaning you hit your clinical endpoint at an earlier stage. This has significant implications for the design and likely successful outcomes of CKD trails. Unfortunately, CKD does not decline in a step-wise manner which is a significant limitation of this approach. Steady loss of function over time is a relatively late manifestation that reflects physiological factors in remnant nephrons. The applicability of 40% decline in eGFR is not uniform across all clinical settings, particularly if the treatment effect is not uniform across those who progress rapidly and those who do not progress. The use of different equations for determining eGFR must also be consider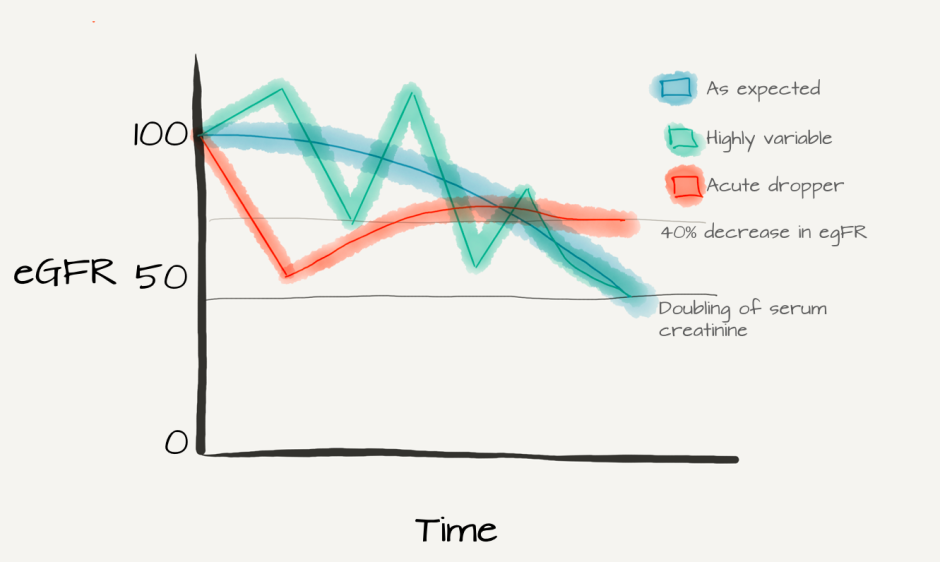 ed. The NKF-FDA concluded that 40% eGFR decline is broadly acceptable as a kidney end point across a wide baseline of eGFR range, however a minimum follow up of 2-3 years is recommended. The trade-off is between improving power (more events) while increasing type 1 error (i.e. false positives).It is important to bear in mind that both contenders are based on a biomarker; they do not provide information regarding patient health status. Creatinine itself has limits as a biomarker; changes in serum creatinine can be attributed not only to renal structural changes but may also be reflective of muscle mass, dietary changes, changes in renal tubular secretion of creatinine (particularly in patients with proteinuria and hypoalbuminaemia), and haemodynamic effects (particularly relevant given how many of our “go to” medications in CKD exert their clinical effects).The chatter so far seems to be leaning towards 40% eGFR decline:Scouting report @methodsmanmd
ed. The NKF-FDA concluded that 40% eGFR decline is broadly acceptable as a kidney end point across a wide baseline of eGFR range, however a minimum follow up of 2-3 years is recommended. The trade-off is between improving power (more events) while increasing type 1 error (i.e. false positives).It is important to bear in mind that both contenders are based on a biomarker; they do not provide information regarding patient health status. Creatinine itself has limits as a biomarker; changes in serum creatinine can be attributed not only to renal structural changes but may also be reflective of muscle mass, dietary changes, changes in renal tubular secretion of creatinine (particularly in patients with proteinuria and hypoalbuminaemia), and haemodynamic effects (particularly relevant given how many of our “go to” medications in CKD exert their clinical effects).The chatter so far seems to be leaning towards 40% eGFR decline:Scouting report @methodsmanmd Mark’s Bracketology for Trial Outcomes @drpaddymark
Mark’s Bracketology for Trial Outcomes @drpaddymark 40% eGFR Decrease and Other New Kids on the Block @Badves
40% eGFR Decrease and Other New Kids on the Block @Badves Combing through previous tweets by @NephRodby:
Combing through previous tweets by @NephRodby:
 Unfortunately, I was unable to uncover any clues about how the rest of the BRP would be inclined to vote based on their Twitter accounts and PubMed searches; perhaps because these aren’t the easiest of search terms to track.Prediction—40% reduction in eGFR purely from the point of view of causing a minor upset of an established behemoth and generating discussion.
Unfortunately, I was unable to uncover any clues about how the rest of the BRP would be inclined to vote based on their Twitter accounts and PubMed searches; perhaps because these aren’t the easiest of search terms to track.Prediction—40% reduction in eGFR purely from the point of view of causing a minor upset of an established behemoth and generating discussion. 
 The second match-up in this region is genuinely intriguing—two diametrically opposed surrogate measures.ProteinuriaBeyond any doubt, proteinuria is predictive of an increased risk of progressive renal function loss over time. This association is found in various pathophysiological conditions, includi
The second match-up in this region is genuinely intriguing—two diametrically opposed surrogate measures.ProteinuriaBeyond any doubt, proteinuria is predictive of an increased risk of progressive renal function loss over time. This association is found in various pathophysiological conditions, includi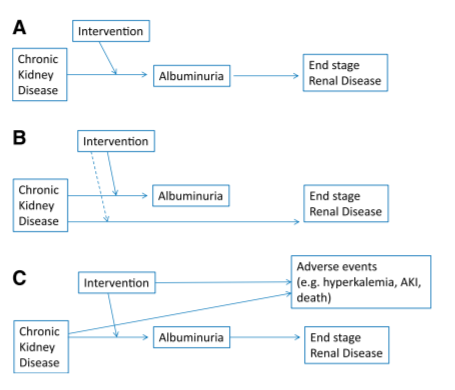 ng diabetic nephropathy, hypertensive nephropathy, and various primary renal diseases. Difficulties arise with regards to 1. Standardised collection methods (spot vs 24 hr collection) 2. Whether it can be used as a surrogate marker—secondary analysis of the RENAAL study found that reduction of proteinuria was a strong predictor of outcome however there are several studies with conflicting outcomes.Patient reported outcomes“The good physician treats the disease. The great physician treats the patient who has the disease” William Osler
ng diabetic nephropathy, hypertensive nephropathy, and various primary renal diseases. Difficulties arise with regards to 1. Standardised collection methods (spot vs 24 hr collection) 2. Whether it can be used as a surrogate marker—secondary analysis of the RENAAL study found that reduction of proteinuria was a strong predictor of outcome however there are several studies with conflicting outcomes.Patient reported outcomes“The good physician treats the disease. The great physician treats the patient who has the disease” William Osler Given its chronicity and symptom burden, the subjective patient experience is key in understanding the impact of CKD. The success of treatments has been historically assessed by doctors using laboratory measures; incorporation of patient perspective into routine clinical practice has been slow to be incorporated. This is because such measures are thought to be intangible and therefore difficult to replicate across clinical trials.
Given its chronicity and symptom burden, the subjective patient experience is key in understanding the impact of CKD. The success of treatments has been historically assessed by doctors using laboratory measures; incorporation of patient perspective into routine clinical practice has been slow to be incorporated. This is because such measures are thought to be intangible and therefore difficult to replicate across clinical trials.
- Patient Reported Outcome Measures (PROMs)—any metric assessing health, illness or health care benefits from the patient's perspective; in general they take the form of a questionnaire. PROMs have the potential to highlight relevant symptoms and changes in symptoms, promote patient engagement in their treatment. They include the Kidney Disease Quality of Life Short Form and the Dialysis Symptom Index.
- Patient-reported experience measures (PREMs) capture information about the healthcare experience as perceived by the patient. They can refer to a variety of issues ranging from cleanliness of facilities to waiting times and how HCPs deliver information.
Of the two, proteinuria has certainly generated the most discussion to date 
 The rest of the BRPGiven the extensive patient advocacy work by @FionaCLoud I would imagine she would lean towards PROs.During her time as ASN President @EleanorLederer has spoken about patient engagement and its role in clinical decision making.
The rest of the BRPGiven the extensive patient advocacy work by @FionaCLoud I would imagine she would lean towards PROs.During her time as ASN President @EleanorLederer has spoken about patient engagement and its role in clinical decision making. @DrDeidraCrews was involved in a study examining patient related outcomes and has done extensive work on social determinants of health.
@DrDeidraCrews was involved in a study examining patient related outcomes and has done extensive work on social determinants of health. Scouting report @methodsmanmd
Scouting report @methodsmanmd Mark’s Bracketology for Trial Outcomes @drpaddymark
Mark’s Bracketology for Trial Outcomes @drpaddymark My prediction: Although proteinuria remains the more controversial of the two, Patient Related Outcomes by a narrow margin (5 to 4).Final winner: 40% reduction in GFR. This could be the dark horse of the competition.
My prediction: Although proteinuria remains the more controversial of the two, Patient Related Outcomes by a narrow margin (5 to 4).Final winner: 40% reduction in GFR. This could be the dark horse of the competition.