#NephMadness Choosing Wisely Campaign (#NCWC) - #HyponatremiaRegion
(aka What Did I Get Myself Into?)Welcome to the #HyponatremiaRegion of #NephMadness - where everything’s somewhat made up and the only the points from the #BlueRibbonPanel matter!
European VS US Hyponatremia Guidelines
Hyponatremia strikes a frisson of anxiety in me, especially when receiving phone calls from colleagues who regard me (as a representative of the nephrology team) as the ultimate authority in the matter. After going through the patients’ medications and history, I generally weakly advise mostly fluid restricting, occasionally fluid resuscitating and, when the mood strikes - investigating for SIADH. For anything else - there is always 3% hypertonic saline (which I have never been successful at obtaining)This is why I leapt at the chance of learning more about how the experts approach this nebulous entity - enter the Battle of the Continents: the European vs US Guidelines! Reading this excellent and concise scouting report by Swapnil Hiremath (@hswapnil) will make navigating the guidelines less daunting.In addition, here is an infographic that attempts to simplify things further: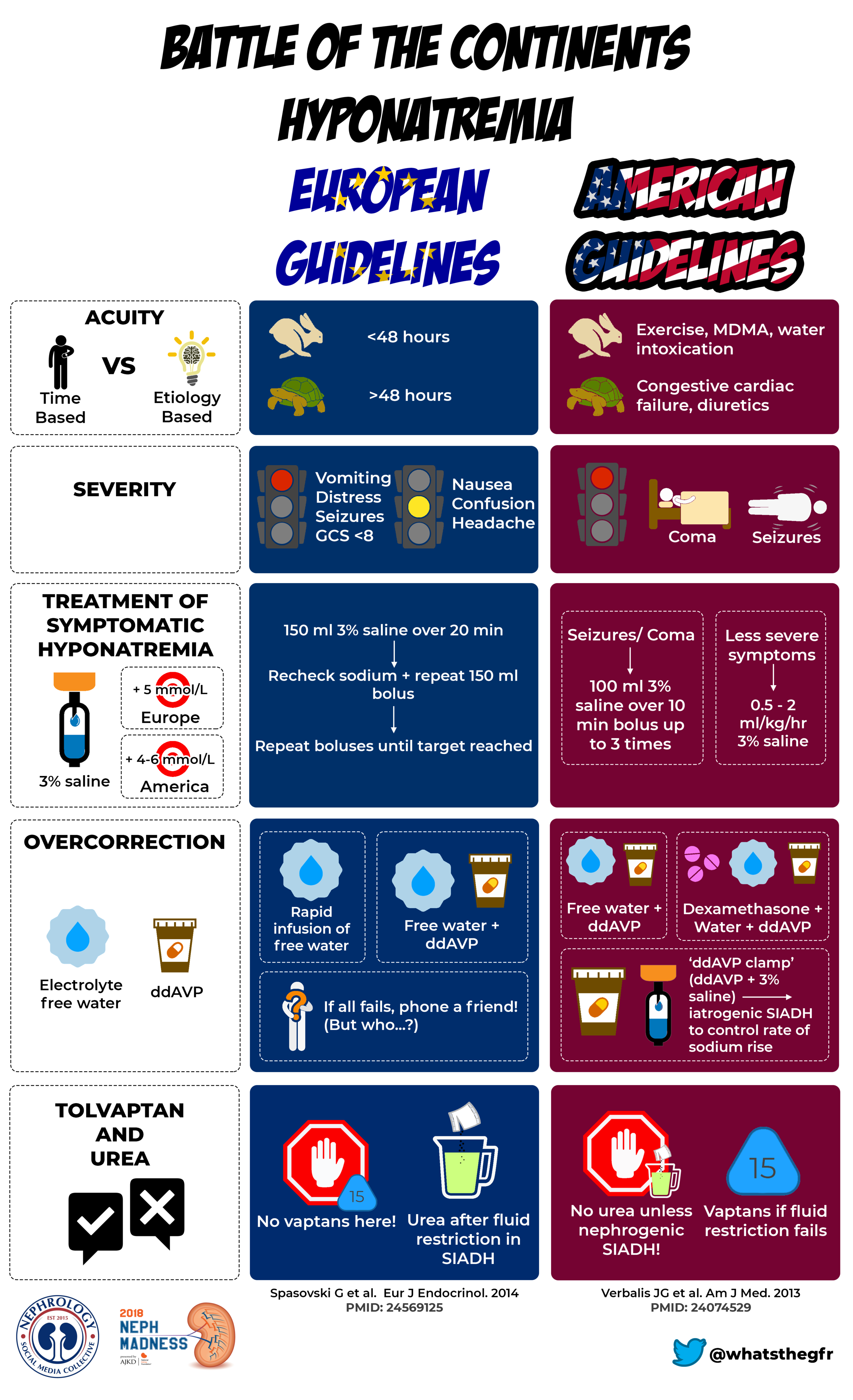 As Swap points out, there are similiarities in the guidelines:
As Swap points out, there are similiarities in the guidelines:
Perhaps the most important part is that both guidelines agree on a limited daily increase in serum sodium even in severely symptomatic hyponatremia (unlike in the 1980s, when the target was to bring sodium up to 128 mmol/L in a day)! And hypertonic saline is the fastest way to fix it on both sides of the Atlantic, as it has been since 1938.
However, he also points out some significant differences:
Do you prefer the Europeans with their streamlined and graded algorithmic advice or the Americans with detailed explanations and ungraded boxes of advice? Do you agree with trials of tolvaptan that results in a recommendation against their use and case series driving a urea recommendation or do you think the funding source and a tolvaptan recommendation are uncomfortably aligned?
Below are screenshots from both guidelines detailing their funding and COI of the authors: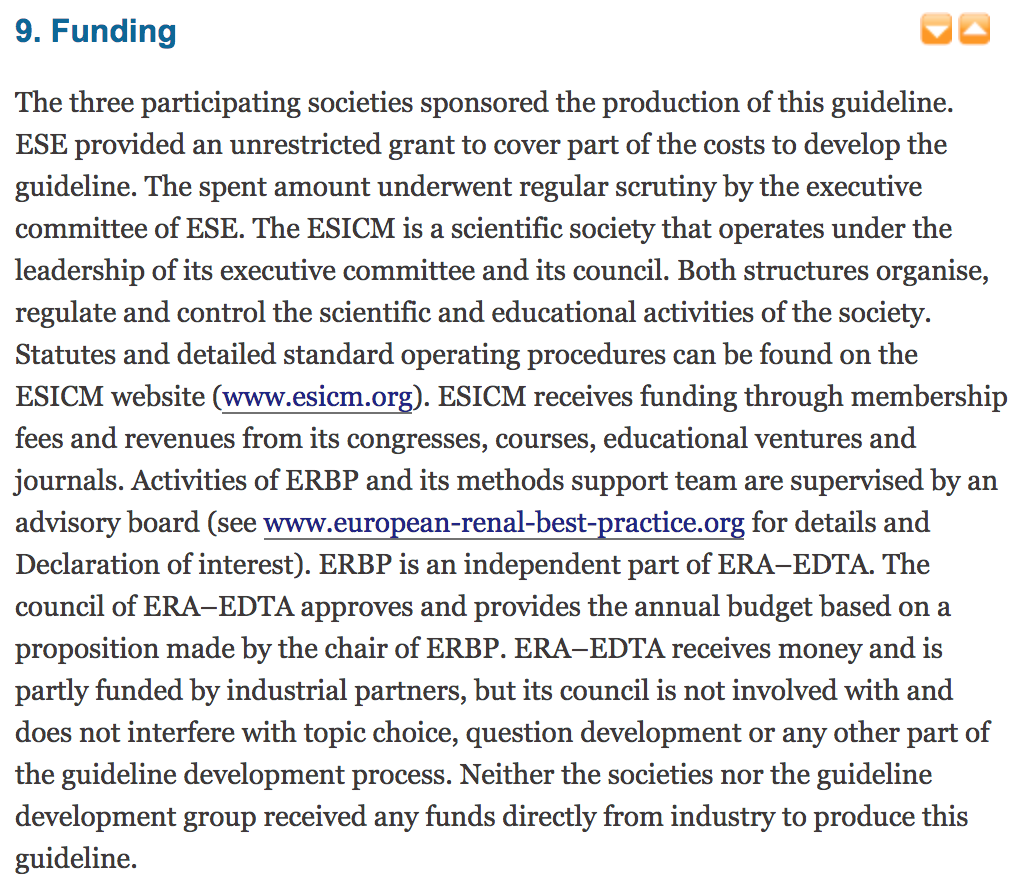
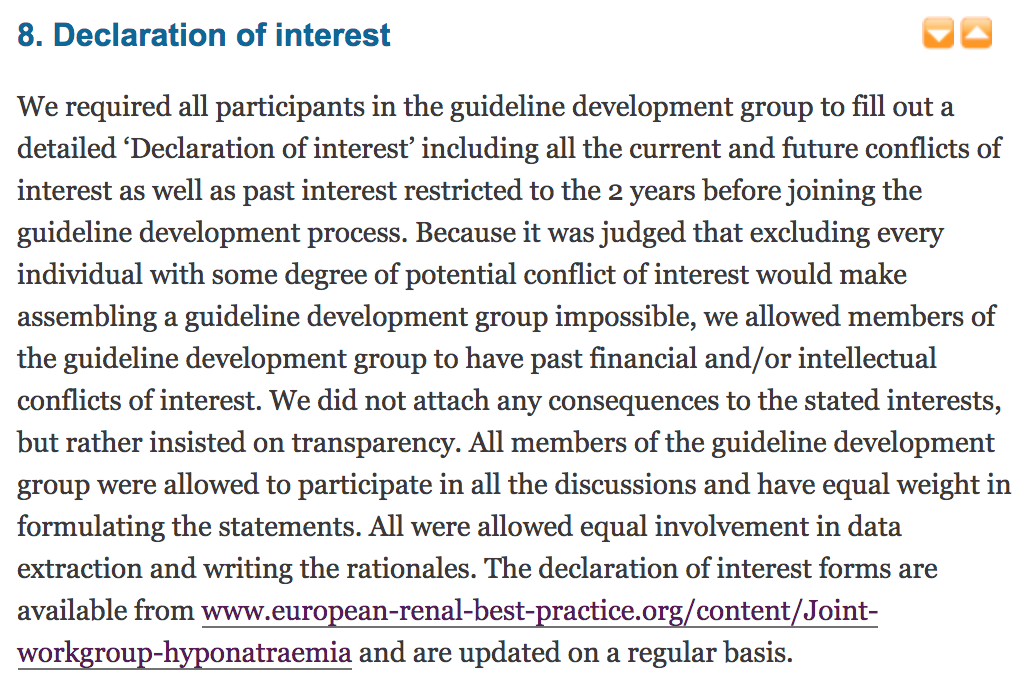
The European Guidelines
The US guidelines
Make of them what you will.A very timely poll by fellow NSMC co-intern Mya Hwte Nge (@mhtwenge) shows what the general public think… but will this reflect the decision of the BRP?https://twitter.com/mhtwenge/status/974845755922907136I started by going through the Twitter accounts of the BRP, and found these from Roger Rodby (@NephRodby) and Mark Reid (@medicalaxioms):https://twitter.com/NephRodby/status/862108529511075840https://twitter.com/NephRodby/status/944331205301952512https://twitter.com/medicalaxioms/status/968654732301557762Unfortunately, I was unable to uncover any other telling clues about how the rest of the BRP would be inclined to vote based on their Twitter accounts and PubMed searches (I did, however, manage to get distracted by quite a few interesting abstracts, so it’s a win-win for me!)I then decided to change my tactic by attempting to dig through the archives of a few other notable salt whisperers and electrolyte gurus who might influence the choices of the BRP: Joel Topf (@kidney_boy - I had to limit myself to tweets from the past 5 years), David Goldfarb (@weddelite), Rush Nephrology (@Rush_Nephrology) , and Bill Whittier (@TWhittier_RUSH). Although not much was found after searches of most of these accounts, the treasure trove of tweets from Joel did not disappoint - it’s safe to say that he is a proponent of vaptans! https://twitter.com/kidney_boy/status/822895568846540801(and he loves a bit of hyponatremia!)https://twitter.com/kidney_boy/status/609013880866664448https://twitter.com/kidney_boy/status/476542619032756224https://twitter.com/kidney_boy/status/476546448247771137(check out the rest of the thread in which he stated Ure-Na worked for him)Disappointingly, I was also unable to clarify Swap's stance on these guidelines - unsurprising, as the scouting report was very balanced and neutral.My last ditch attempt at trying to get somewhere with this ended with me going through some open forum posts at ASN communities. I get the feeling that both tolvaptan and urea are favoured by nephrologists, but with the caveats that:
- Tolvaptan costs a lot more, and there are a few articles that highlight the possibility of osmotic demyelination syndrome with overly rapid correction of hyponatremia (here, here and here) - hence the need for very close monitoring and careful dosing
- Urea is potentially unpalatable - although this might be debunked with this viral tweet of Roger trying some Ure-Na:
https://twitter.com/NephRodby/status/889225627135610880I feel that the BRP (maybe besides Mark) will be inclined to vote for the US guidelines - why not have two weapons in your arsenal, rather than be limited to just one? Does it matter greatly that Otsuka funded the US guidelines when other prominent nephrologists who don't seem to have conflicts of interest swear by vaptans?
SIADH VS Cerebral Salt Wasting (CSW)
Swap succinctly explains why these two entities are important to distinguish in his scouting report:
In SIADH, the first-line intervention is fluid restriction, which will make matters worse in the volume-contracted patient with salt wasting. Conversely, salt wasting syndromes can be easily fixed with intravenous normal saline, which would make hyponatremia worse if the patient has SIADH instead.
He tries his best to stay impartial throughout the description of cerebral salt wasting, but then ends the section with this:
Regardless of what you think about the reality of cerebral salt wasting, SIADH is a condition that every nephrologist worth their salt needs to know how to manage. It is not an easy condition to deal with. Clinicians need to use all their cerebral capacity to recognize symptoms, correct the sodium level with the appropriate level of aggressiveness, and not spend too much time chasing the salt-wasting hobgoblins.
I struggled to find any opinions on cerebral salt wasting by the BRP bar this one by Roger...https://twitter.com/NephRodby/status/889239264378093569 But then this impassioned thread by David in response to Mitch Rosner’s picks for the #HyponatremiaRegion dropped - and it looked like the final word on CSW had been said! @weddellite for CSW!https://twitter.com/weddellite/status/975510380322672641I did not think that this would have gone unchallenged - what did the rest of NephTwitter think? Check this thread out!https://twitter.com/kidney_boy/status/976450800867270657(tl;dr - Joel and Matt Sparks, @Nephro_Sparks are decidedly not backing CSW)I therefore predict that this will actually be an upset and the BRP will vote for CSW (with the possible exception of Roger who might not take the outcome without a fight - might this herald internal disharmony among the BRP?!)In conclusion, I feel that the two winners of this unassumingly controversial bracket will be the US guidelines and cerebral salt wasting!Follow #NCWC for region updates.Read the full AJKD blog (and check out the full scouting report for the #HyponatremiaRegion here).Submit your NephMadness brackets here.