#NephMadness Choosing Wisely Campaign - (#ContrastRegion)

Contrast is Nephrotoxic vs Contrast is NOT Nephrotoxic
Contrast Induced Nephropathy (CIN) or Contrast Induced AKI (CI-AKI) or may be Contrast Associated AKI (CA-AKI) surely exists. It may be wrongly diagnosed using the serum creatinine elevation definition, or it may be over-diagnosed with lots of associations and comorbidities. However, it does exist and we all saw patients, even "dialyzed" patients with CI-AKI. As written on the AJKD blog:
Raise your hand if you have seen a patient with AKI due to contrast administration (and if you didn’t raise your hand, either you are not a nephrologist, or, ahem, you need to brush up on your diagnostic acumen!).
Even the writer of "Contrast is NOT nephrotoxic" section still has some doubts:
We repeat, association is not causation. To call AKI in a patient with vascular disease, sepsis, underlying CKD, who, by the way, has had a recent contrast-enhanced computed tomography (CT) scan, as contrast-induced is just plain lazy! Hence there has been a move afoot to replace CI-AKI to contrast associated AKI (CA-AKI), or even post-contrast AKI. But with so many associations, surely there is fire beneath the smoke?
Moreover, the selection committee member Prof. Paul M. Palevsky, one of the co-authors of the famous recent PRESERVE trial, still think that IV contrast has a risk for nephrotoxicityhttps://twitter.com/PaulPalevsky/status/935968679874920449However, neither Dr Palevsky, nor others who wrote this excellent AJKD blog post; Swapnil Hiremath (@hswapnil), Anitha Vijayan (@VijayanMD), Natasha Dave (@NatashaNDave), and Rajeev Raghavan (@jeevsmd), will choose which of the 2 brackets will win.Let's dig deeper into the actual #BlueRibbonPanel (BRPs) Twitter feeds/PubMed searches to see if that reveals the possible picks:Doing a Twitter search with (each of their account names + contrast) gave positive results for 2 of the BRP; Roger Rodby @NephRodby and Mark Reid @medicalaxiomsDr Rodby tweeted something about CIN deniers:https://twitter.com/NephRodby/status/886381890072084480The Mark Reid Twitter search didn't bring up a clear statement about nephrotoxicity, but in general he seems an advocate for nephrotoxicity.This is 2/9 for Contrast Nephrotoxicity.Searching Pub ed for other BPR members:Dr Sarah Faubel, is an expert in AKI, her PubMed search identified many articles about deleterious effects of AKI including CI-AKI. So, she probably would also vote for Contrast nephrotoxicity. Dr Fiona Loud is one of the contributors to the NICE AKI guidelines in 2014, which clearly discusses the CI-AKI issue.No clear statement about contrast being non-nephrotoxic from any of the BRP members.This leaves us with 4 (out of 9) members possibly voting for Contrast is Nephrotoxic, with the 5 others also will probably do the same!A follow up AJKD blog post by Dr. Michael Rudnick confirmed our results, when he stated clearly that:
Verdict: Contrast IS nephrotoxic among high-risk patients. We would consider it a technical foul against the nephron if the threat of CI-AKI is not considered in patients with an eGFR < 30 mL/min and in patients with eGFR 30-44 mL/min, especially if coupled with high risk features such as diabetes
Gadolinium in CKD4 vs Iodinated Contrast in CKD4
If you choose to go with contrast is not nephrotoxic, you would probably choose Iodinated contrast in CKD4, however, as we concluded above, Contrast is Nephrotoxic, so we will argue for Gad in CKD4.The AJKD blog post is killing it with some straightforward statements we are highlighting here:
What about doing a contrast-enhanced CT scan, using iodinated agents instead? Even the most avowed obituarist of CA-AKI will still accept that there is a risk of AKI after contrast when the eGFR is already so low. A small rise of 25%-50% in Scr may be all you need to push the CKD stage 4 patient over the edge. The resultant oliguria and fluid overload will quite often necessitate starting dialysis. Immediately. Weigh that against the very small (likely <<<1%) lifetime, long-term risk of NSF with the lower risk group II agents. The choice will light up brighter than any contrast agent.
Also:
In conclusion, to quote the European guidelines, “An unfortunate result of anxieties about NSF has been that enhancement during MRI may be avoided inappropriately and important disease overlooked. In a patient with mild or moderate renal impairment, the risk of NSF from an MR examination enhanced with one of the most stable gadolinium-based agents is likely to be less than the risk of nephrotoxicity from a CT examination enhanced with an iodine-based agent.”
Even when arguing for iodinated contrast in CKD4, they ....
Estimates of contrast use, from 2003, were 80 million doses, corresponding to 8 million liters of iodinated contrast in humanity. If you are a strong believer in contrast causing kidney failure, this volume of contrast could explain the entire CKD epidemic!
Probably it is Swapnil (@hswapnil), who seems not convinced at all with the non-nephrotoxic contrast!https://twitter.com/hswapnil/status/975125791036993536So, how about the BPRs thoughts (I mean that is what we all want to know anyway?A rapid look at Twitter and PubMed, will not result in much info, except for Roger Rodby, who wrote an opinion paper about the use of Gad in HD concluding clearly that: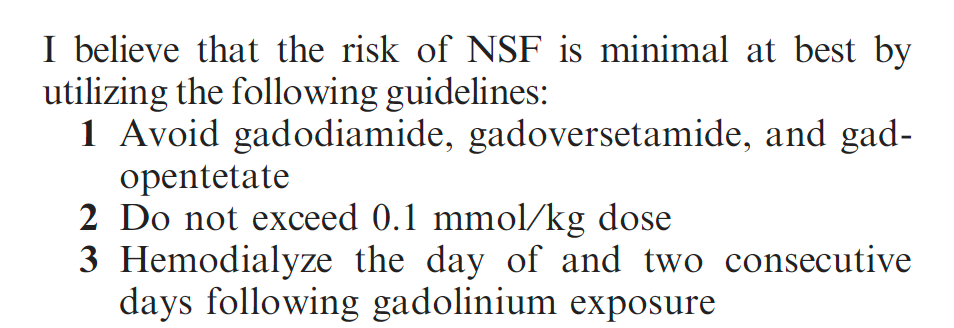 And those of you who are following ASN Communities, will know his opinion regarding this issue.We presume that other BRP member who will vote for Contrast is Nephrotoxic, will also vote for Gad in CKD4 (or maybe not). But these are the available data currently.See you in another region.Follow #NCWC for daily region updates.Read the full AJKD blog (Contrast region) here .Submit your NephMadness brackets here.
And those of you who are following ASN Communities, will know his opinion regarding this issue.We presume that other BRP member who will vote for Contrast is Nephrotoxic, will also vote for Gad in CKD4 (or maybe not). But these are the available data currently.See you in another region.Follow #NCWC for daily region updates.Read the full AJKD blog (Contrast region) here .Submit your NephMadness brackets here.